Abstract
Background: The aim of this study was to assess the effect of wrist tapping (WT), according to the author’s method, on the synchronization of alpha activity in healthy adults and patients with juvenile myoclonic epilepsy (JME).
Methods and Results: The study included 71 people of working age, including 51 clinically healthy volunteers (median age — 39[21;56] years) and 20 patients with JME (median age 27[23;35] years). Under the influence of WT in a state of sensory deprivation, statistically significant changes in the alpha peak frequency (APF) (P<0.001) and alpha power (AP) (P<0.05) were found in healthy adults. In JME patients, there were statistically significant changes in the APF (P<0.05) and AP (P<0.05), as well as a statistically significant increase in the the alpha range width (P<0.05) after WT. WT, according to the author’s technique, allows reducing the severity of alpha rhythm synchronization and leads to a shift in the peak frequency of the alpha rhythm in the occipital leads towards the alpha-2 sub-frequency range and a decrease in AP in both healthy volunteers and JME patients. At the same time, the alpha range width in the occipital leads is statistically significantly increased in JME patients.
Conclusion: The nature of the change in the alpha rhythm, in comparison with the control, indicates the phenomenon of resonance with the frequency of the WT rhythm. The WT effect testifies to the prospects of the clinical application of WT in JME, since it was previously shown that if the selected external frequencies enter into resonance with the neurons of the antiepileptic system, then an antiepileptic effect could be obtained.
Introduction
Resonance (French resonance, from Latin resono “I respond”) is a frequency-selective response of an oscillatory system to a periodic external influence, which manifests itself in a sharp increase in the amplitude of stationary oscillations when the frequency of an external influence coincides with certain values characteristic of a given system. For linear oscillatory systems, the values of resonance frequencies coincide with the frequencies of natural oscillations, and their number corresponds to the number of degrees of freedom. Under the influence of resonance, the oscillatory system turns out to be especially responsive to the action of an external force. With the help of resonance, even very weak periodic oscillations can be distinguished and/or amplified. Resonant phenomena can lead to both destruction and increased stability of mechanical systems—hence, epileptic systems. External stimuli can provoke epileptic seizures, but if the selected frequencies resonate with the neurons of the antiepileptic system, an antiepileptic effect can be obtained. Currently, the theory of resonance is used more and more widely in neurorehabilitation, when the impact of external stimuli with a certain frequency, which is in resonance with the neuronal activity of defense systems, can have a clinically significant therapeutic effect.(1,2) On the other hand, epileptogenesis is based on a hypersynchronous state of neuronal activity in the epileptic focus. This phenomenon is called secondary bilateral synchronization, a phenomenon that blurs the line between focal and generalized epileptic seizures. Synchronization refers to the simultaneous onset of identical waves under several electrodes in one hemisphere of the brain. Bilateral synchronization is a situation in which identical waves appear simultaneously over the homologous parts of both hemispheres.(3) The development of video-EEG monitoring of epileptic seizures together with neuroradiological research methods have made it possible to establish that a clear division of all epilepsies into generalized and focal epilepsies is an abstraction rather than a clinical reality.
For example, the following facts are well known: focal seizures are present in the structure of generalized epilepsy;(4) focal EEG changes in generalized epilepsy have been detected in 30–35% of all cases;(5) focal structural abnormalities are present in IGE;(6) the frontal lobes play a leading role in the pathogenesis of such a form of epilepsy as JME.(7) In IGE, where the frontal cortex plays a leading role in the development of generalized activity, the effect of hypersynchronous neuronal activity is a possibility.
Thus, using the theory of resonance and hypersynchronous neuronal activity, we can, by external influence at certain frequencies, desynchronize neurons in the focus of epileptic activity, achieve the phenomenon of resonance with neurons of the antiepileptic system and reduce the risk of developing generalized and secondary generalized seizures.
In recent years, not only drug-based, but also non-drug methods of epilepsy therapy have been actively studied,(8) among which the method of WT is of great interest;(9) this method leads to a decrease in the severity of anxiety both in healthy volunteers and in patients with epilepsy.(10) However, we have not found any works that study the effect of carpal tapping on the severity of alpha rhythm synchronization, either in healthy people or in patients with epilepsy. Such a study would undoubtedly be of scientific and clinical interest.
The aim of this study was to assess the effect of WT, according to the author’s method, on the synchronization of alpha activity in healthy adults and patients with JME.
Materials and Methods
The study included 71 people of working age, including 51 clinically healthy volunteers (median age — 39[21;56] years) and 20 patients with JME (median age 27[23;35] years).
All participants underwent EEG while subjects were sitting in a dark room, fully awake but with the eyes closed. The following are the parameters of the alpha rhythm in the occipital leads (O1, O2): the alpha peak frequency (APF, Hz), the alpha range width (ARW, Hz), and the type of peak of the alpha rhythm (monopeak, beepeak, polypeak). In addition, the alpha rhythm power (AP, μV2) in the occipital leads was analyzed. The above characteristics of the alpha rhythm were recorded before the manual tapping technique and during the first three minutes after its completion. EEG recording was carried out in a state of sensory (visual and sound) deprivation.
The study of the WT was carried out according to the author’s modified methodology, “Method of exogenous rhythmic stimulation influence on an individual human rhythm” [RF patent No2606489 of 10.01.2017]. Modification of the method included carrying out the study of the patients’ individual rhythms without the use of exogenous rhythmic stimulation. The study was conducted in the morning with the exclusion of external sensory stimuli (loud sound, bright light) and other people, except the doctor and the volunteer, during the tapping procedure. The temperature regime of the environment was maintained within the range of 22-25 oC. WT was done with eyes closed. The technique involved wrist tapping on the surface of the device (Android smartphone), followed by the registration of the time parameters of this process in the original program based on the modified technique “Method of exogenous rhythmic stimulation influence on an individual human rhythm.” During the task performance, the mechanogram where vertical strokes display the contact of the finger with the screen appears on the screen of the device.
Inclusion criteria for the main group:
— Patients with JME
— Signed voluntary informed consent
— Male and female
— The age period: the youth (males 17-21; females 16-20
years); the first period of middle age (males 22-35 years; females 21-35 years); the second period of middle age (males 36-60 years; females 36-55 years)
— Russian-speaking Europeans
Inclusion criteria in the control group:
— Healthy adults
— Signed voluntary informed consent
— Male and female
— The age period: the youth (males 17-21; females 16-20
years); the first period of middle age (males 22-35 years; females 21-35 years); the second period of middle age (males 36-60 years; females 36-55 years)
— Russian-speaking Europeans Exclusion criteria:
— Children and adolescents
— Refusal to participate in this study
— Participation in other studies
— Acute and chronic neurological, psychiatric and
endocrinological disorders at the time of examination
— Alcohol intake (2 or more drinks during the last 2 weeks) — Use of narcotic drugs at the time of the study and in history
Volunteers did not receive any payment for participating in this study. The researchers did not receive any payment for conducting the study.
Statistical processing was carried out using the STATISTICA Version 10 (StatSoft, USA). The normality of distribution of continuous variables was tested by Shapiro- Wilk test. Median (Me), interquartile range (IQR; 25th to 75th percentiles) were calculated. The Wilcoxon test was used to compare differences between two dependent groups. A value of P
Results
Under the influence of WT in a state of sensory deprivation (Table 1), statistically significant changes in the APF (P<0.001) and AP (P<0.05) were found in healthy adults. The majority of the subjects (70.6%) showed a change in the peak characteristics (Table 2), of which 43% showed its splitting and transformation into polypeak, and 27.4% — a decrease in the number of peaks. Only 29.4% of subjects presented no changes in the peak characteristics.
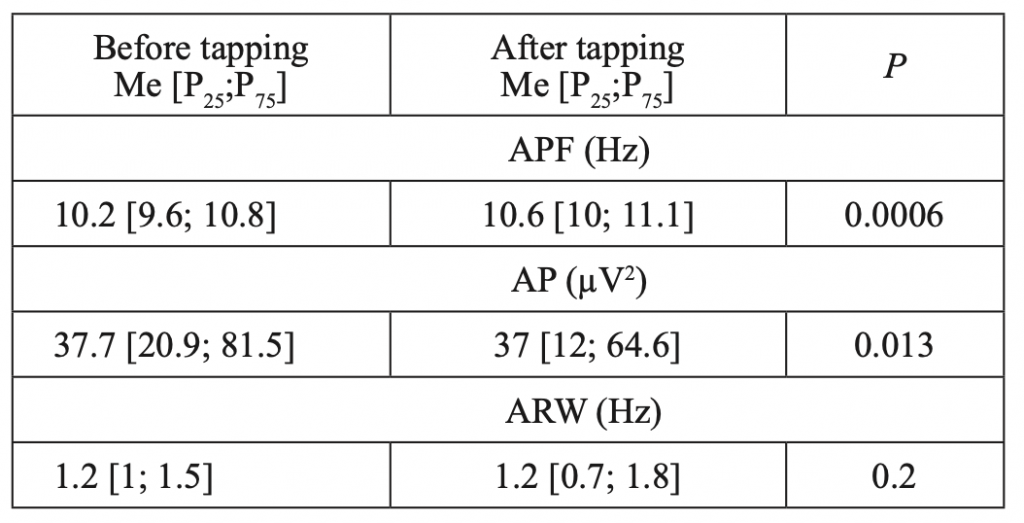
Table 1.
Characteristics of alpha rhythm before and after WT in healthy adults (n=51)
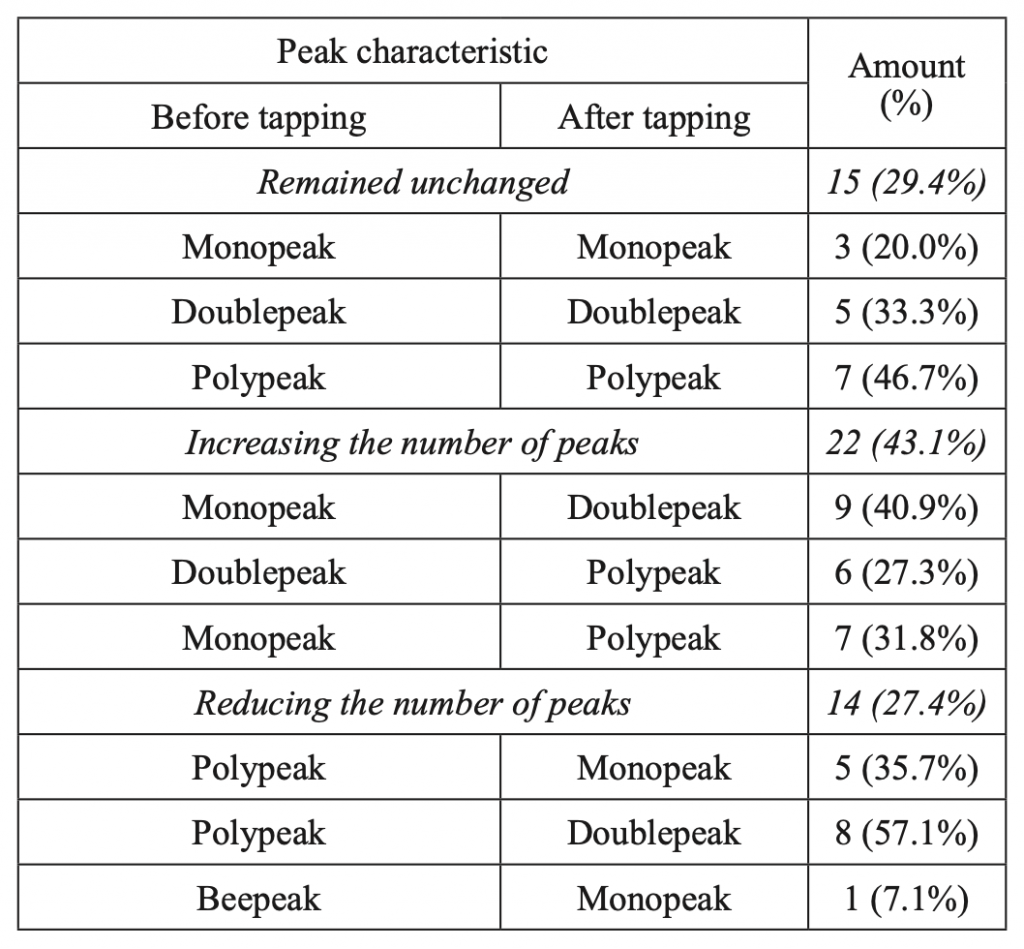
Table 2.
Changes in the characteristics of the alpha-rhythm peak in the occipital leads before and after WT in healthy adults (n=51)
In JME patients, there were statistically significant changes in the APF (P<0.05) and AP (P<0.05), as well as a statistically significant increase in the ARW (P<0.05) after WT (Table 3). The majority of the subjects (75%) showed a change in the peak characteristics (Table 4), of which 35% showed splitting and transformation into polypeak, and 40% - a decrease in the number of peaks. Only 25% of subjects presented no changes in the peak characteristics.
[caption id="attachment_263" align="alignnone" width="870"]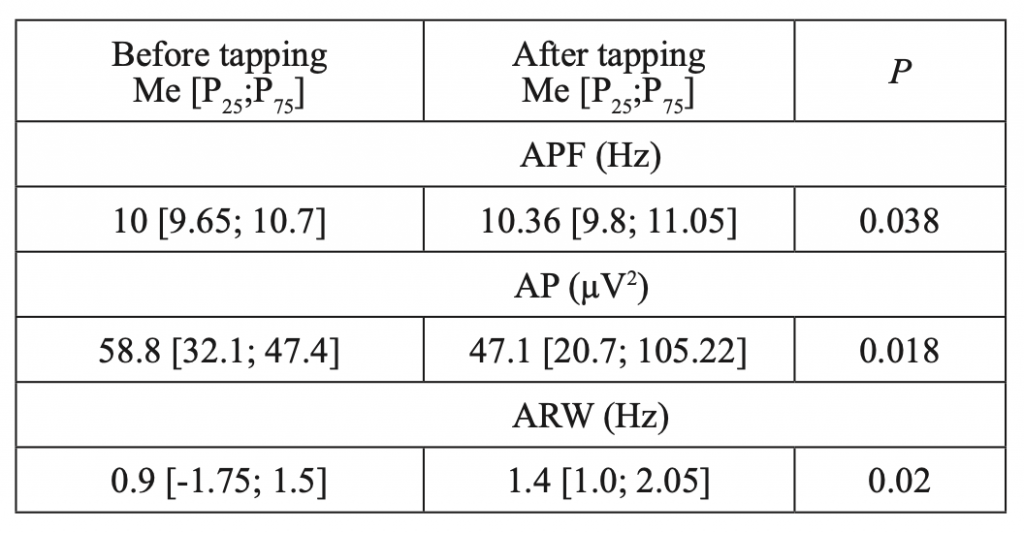 Table 3.
Table 3.
Characteristics of alpha rhythm before and after WT in patients with JME (n=20)[/caption]
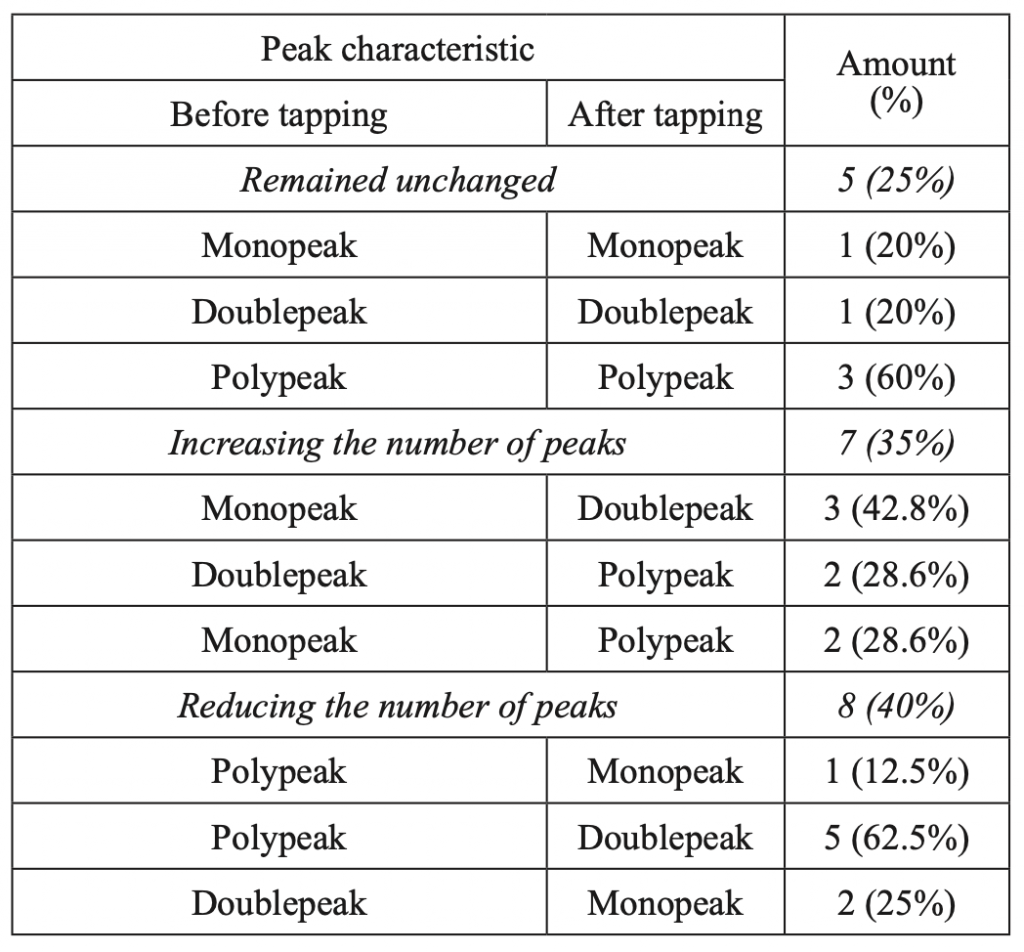
Table 4.
Changes in the characteristics of the alpha-rhythm peak in the occipital leads before and after WT in patients with JME (n=20).
Discussion
The main regulator of biorhythms and the life processes they cause is the brain,(11) the biorhythm of which is associated with the individual characteristics of self-regulation mechanisms and the level of plasticity of neurodynamic processes.(12) Considerable attention is paid to the study of the synchronization of various parts of the cerebral cortex in the processes of regulation, primarily in the range of alpha and beta rhythms, and to changes in the functional state of the body.(13,14) Targeted studies of fMRI in patients with epilepsy have shown that the functional resting networks of the brain fluctuate on a scale from a second to a minute.(15,16) Thus, the concept of dynamic functional connections is an important aspect of the functional activity of the brain at rest, which looks at variations in functional connectivity over a short period of time. Analysis of dynamic functional connections showed that spontaneous transitions between networks of interacting regions of the brain are highly organized into a hierarchy of two types of meta states: one for cognitive systems of a higher order, and the other for sensorimotor systems.(17) Several studies have shown hyperdynamic activity in some specific functional networks at rest in various subtypes of epilepsy.(18) Aberrant dynamics of functional connections at rest was also observed in IGE with GTCS,(19) but many questions remain not fully understood. Previous studies have provided ample evidence to support the hypothesis that IGE, and JME in particular, is multiregional thalamocortical “network” form of epilepsy,(20) rather than generalized epileptic disorder. In addition, stationary connectomic correlations with cognitive impairment have been found in the thalamo-motor and thalamo-frontal system.(21,22) However, it remains largely unclear whether there is a deficit in dynamic interactions between functional resting networks in JME. The processes of synchronization of the bioelectric activity of the brain in various physiological and pathological states of the body in active wakefulness and in relaxation, as well as in JME, have not been sufficiently studied. A comprehensive study of the processes of synchronization of brain biorhythms, both at rest and with external (exogenous) stimuli, would contribute to the understanding of the processes by which the plasticity of nervous processes and the regulatory function of the brain develop.
In conclusion, wrist tapping, according to the author’s technique, allows reducing the severity of alpha rhythm synchronization and leads to a shift in the peak frequency of the alpha rhythm in the occipital leads towards the alpha-2 sub- frequency range and a decrease in AP in both healthy volunteers and JME patients. At the same time, the alpha range width in the occipital leads is statistically significantly increased in JME patients. The nature of the change in the alpha rhythm, in comparison with the control, indicates the phenomenon of resonance with the frequency of the WT rhythm. Taking into account excessive synchronization of large neuronal populations leading to a hypersynchronous state in epilepsy, the technique we have developed can be promising as a method of non-drug therapy and/or prevention of the development of generalized and secondary generalized epileptic seizures on stages of the aura or simple focal epileptic seizures. The WT effect testifies to the prospects of the clinical application of WT in JME, since it was previously shown that if the selected external frequencies enter into resonance with the neurons of the antiepileptic system, then an antiepileptic effect could be obtained. However, confirmation of our hypothesis requires further study with the inclusion of a sample of patients suffering from focal and generalized forms of epilepsy.